
Peripheral neuropathy is a frequent cause of pain in the hands and feet. This widespread discomfort and nerve damage can result from diabetes, chemotherapy, or any condition that reduces the energy supply or function of small nerves near the skin’s surface. However, peripheral neuropathy is not the only cause of extremity pain. Compression of larger nerves is also common (and underappreciated). I see patients nearly every week whose numbness is diagnosed as peripheral neuropathy and who are told there is nothing else that can be done other than medications for the pain. This is not true. I’ve explored treatment options for peripheral neuropathy in a previous blog post. Nerve compression has more and different possible therapies.
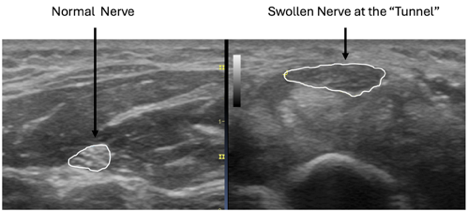
Before treatments can be proposed, however, the diagnosis needs to be clear. Ultrasound is among the most effective diagnostic tools, with images that have improved dramatically over the past decade. We can now see, measure, and evaluate the major nerves of the hands and feet. When a nerve is compressed, it appears swollen and inflamed. This swelling can’t be seen on X-rays and isn’t visible on typical MRI scans. These compressions most commonly occur in areas described as “tunnels,” including the wrist (carpal tunnel), the elbow (cubital tunnel), the forearm (radial tunnel), the foot (tarsal tunnel), and the hip (aponeurotic fascial tunnel). The names vary by location and are sometimes difficult to pronounce, but the effects on the nerve are the same. Compression causes the nerve to malfunction, resulting in numbness and pain. The following side-by-side ultrasound images show a cross-sectional scan of the median nerve in the wrist. The nerve is swollen, nearly double its size at the site of compression.
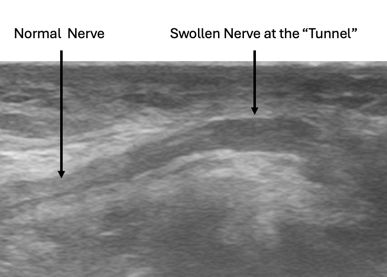
The second image below shows a longitudinal view of the ulnar nerve at the elbow (cubital tunnel). As you can see, the nerve swells as it approaches the tunnel.
Surgery has long been used to treat these nerve compressions but isn’t the only option. Carpal tunnel surgery at the wrist is performed more than 500,000 times per year in the US. Unlike spinal nerves, which are frequently compressed by bone, the peripheral nerves in the arms and legs are compressed by soft tissues. These soft tissues (called fascia) can be expanded using a technique known as hydrodissection.
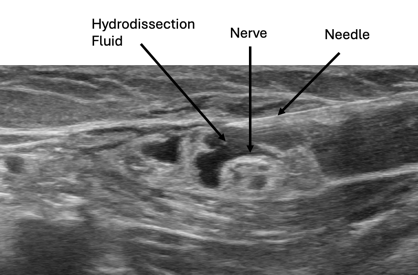
The hydrodissection technique uses fluid and gentle pressure to widen soft-tissue spaces, freeing the nerve and giving it room to breathe. Various fluids can be used for hydrodissection, including dextrose prolotherapy and PRP. Prolotherapy solutions have been shown to reduce pain and swelling in the carpal tunnel more effectively than steroids. PRP also shows good success, especially when growth factors are needed to “jump-start” the functions of a damaged nerve. Research has demonstrated that PRP may have advantages over prolotherapy and steroid injections, especially when there is significant nerve dysfunction. The image below shows how hydrodissection fluid can free the nerve from surrounding soft connective tissue. This technique can also be effective in areas with surgical scar tissue that entraps the nerve.
Once nerve compression is relieved, proteins and nutrients can again reach the nerve's ends. Nerve health is restored, swelling resolves, and pain subsides. Ultrasound has been a remarkable tool for both identifying compressed nerves and guiding non-surgical hydrodissection to restore their function.
If you have pain or numbness in your arms, legs, or other body parts, seek out a practitioner skilled in ultrasound nerve assessment to determine if your symptoms are caused by neuropathy, a trapped nerve, or a different condition. Hydrodissection may provide relief without medication or surgery.

